How we built a Clinical Supply Optimization program at The University of Kansas Health System
At The University of Kansas Health System, “proud but never satisfied” is an ongoing, powerful statement we receive from Bob Page, president & CEO and Tammy Peterman, executive vice president, COO, CNO & president of Kansas City Operations. This statement is also the title for their newly released book of the same name. As vice president of supply chain, I am consistently working through ways in which we can perform at the highest level. I am very proud of the work we have accomplished; however, we always have areas in which we can grow, improve, be more efficient, etc.
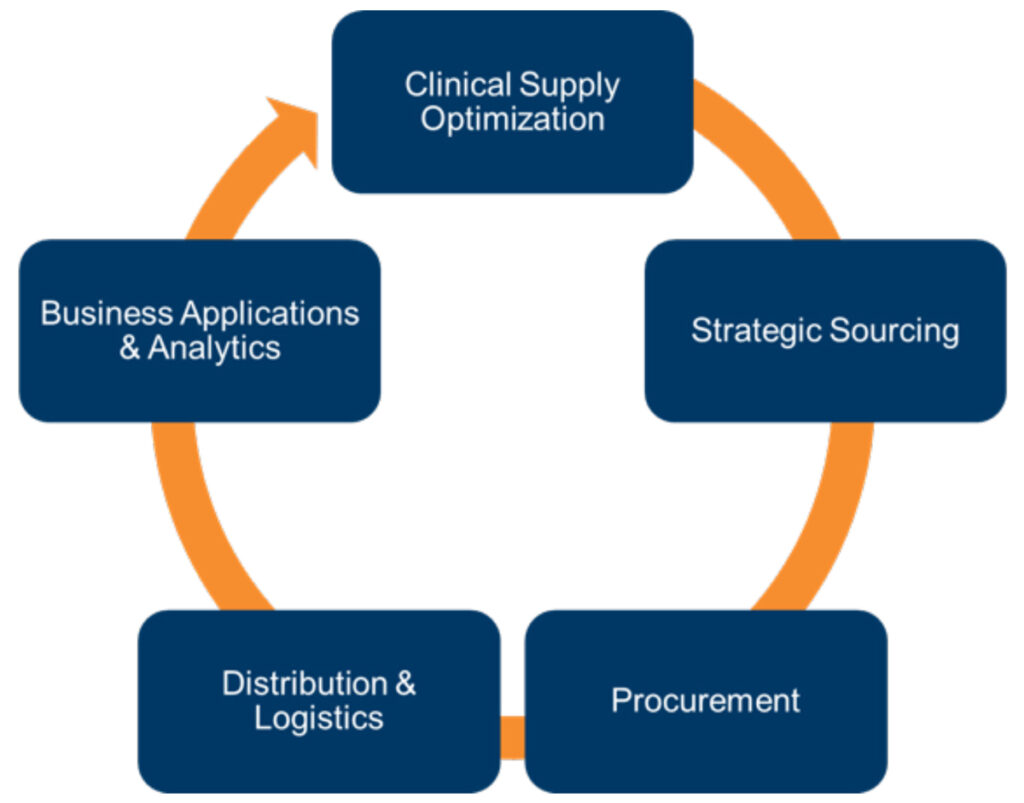
The recent COVID-19 pandemic presented to us an opportunity to really dig deep into value analysis and strategic sourcing based on the immediate need to do business differently to provide crucial supplies for our healthcare system. As we explored our vision, we evolved our program. This is how the Clinical Supply Optimization (CSO) program was born.
My experience having worked over 20 years in the cardiac cath lab and in healthcare supply chain 20 more has taught me that clinician engagement with supply chain is critical. Accomplishing this goal requires a strong team armed with financial data, clinical outcomes and operational data. Once our teams were in place, we implemented an Enterprise Resource Planning (ERP) program system-wide and engaged with a clinical evidence engine that doubles as our project management tool. Our program is a heavily data-driven process which is essential when making supply decisions. It is important to mention that part of our program encompasses a succession plan. We want to leave a legacy and we want most of all to have programs in place that ensure the safety of our patients and staff.
The need for CSO
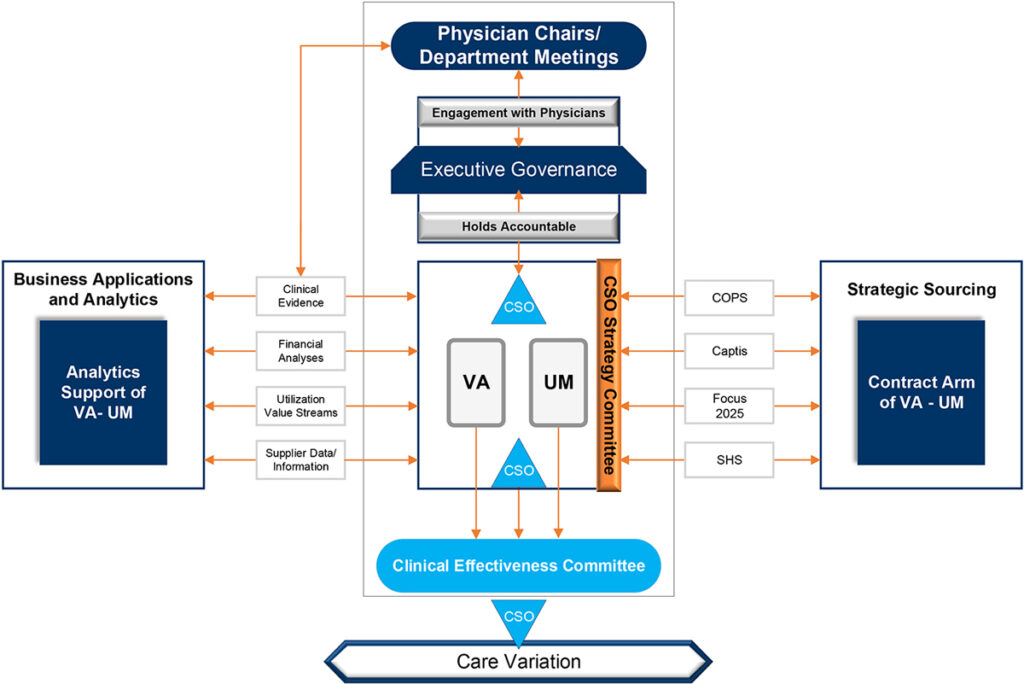
We had a traditional Value Analysis (VA) program that identified ways in which new products would come into the health system. The focus was to purchase products at the right price, though we felt we could do more. As such, we added value streams and implemented a Utilization Management (UM) program that would review purchasing the right products at the right price and at the right time. Once we knew the significant impacts of having both VA and UM programs, we needed a name that was reflective of the total program and its ability to effectively and consistently engage our health system’s clinicians, incorporating clinical evidence into our workflows, and acquiring key financial and operational data to drive decisions. CSO was born out of this work. With this foundation, our CSO team can provide the necessary knowledge to our end-users to make the best decisions on the supplies and medical devices we use to care for our patients today and into the future – all while sustaining healthy business practices to keep our organization in a viable place.
Up and running
Getting the program up and running involved several components:
People. We took time to get the right people in the right role to execute on this work. We moved existing people into open positions. We then created a few new positions and hired for those specifically. Under the direction of Mark Walterbach, system senior director of Supply Chain Management & Administration, these are the members who make up our CSO Team:
Angie Bruns, system director, Clinical Supply Optimization (CSO)
- Chad Derdich, system manager, Value Analysis
- Shannon Maize, system analyst, Value Analysis
- Kim Dyer, system analyst, Value Analysis
- Marissa Muchow, system analyst, Value Analysis
- Lisa Love, system analyst, Value Analysis
- Chris Heath, system manager, Utilization Management
- Jennifer Pellatz, system analyst, Utilization Management
- Erika Mohler, system analyst, Utilization Management
Processes. We created many new policies and procedures to support the advanced program strategy. We then illustrated how each of these processes interweaves within every segment of supply chain.interweaves within every segment
Systems. The University of Kansas Health System spreads beyond just our Kansas City division. In keeping with the Health System’s “One Team” concept, we needed to implement these programs within our Greater Kansas facilities. We implemented Workday for our ERP, ECRI for evidence-based medicine, value analysis and utilization management. We are also using Vizient procedural analytics and clinical database tools.
Communication is paramount
Communication is paramount for any program. Launching the CSO program mandated a complete cultural shift. The key was in fostering a strong, trusting relationship with our clinical leadership. This involved countless meetings with our leadership teams system-wide. We created committees to address solutions for their specific areas. We reached out to multiple venues with multiple people, multiple times to really drive home the need for the program and its advantages. The support we received across the health system was astounding.
Clinical Supply Optimization (CSO) is an ongoing, interdisciplinary strategy that informs decision making to optimize utilization of products or services while eliminating harm, improving outcomes and lowering costs.
Throughout the COVID-19 pandemic we were forced with having to be creative and innovative as we faced challenges with supply shortages and needed to source PPE outside of our traditional supply allocations. This meant we would be bringing in PPE that we hadn’t used previously, and we needed a way to engage our clinicians in finding a suitable solution while maintaining our standards of care.
One of the developments from our CSO program was to create a product formulary of PPE for future PPE shortages. We formed a PPE Test Group with leaders from inpatient units, ED, transport, pharmacy, EVS, RT/PT/OT and procedural areas system-wide. This group takes samples of non-formulary products, such as, ear loop masks, gowns and gloves to frontline staff to trial and provide feedback. Products receiving positive reviews will then go through our Strategic Sourcing team who determines the ability to source these products in bulk as well as review any contracting and financial obligations before moving forward.
Goals and hopes for the program
We want to be a true clinically integrated supply chain, evolving beyond a transactional supply chain. We want physicians at the table making supply chain decisions and we want to have a culture that is mindful of all costs within the organization.
Added value streams through the UM program:
| Utilization | Disease Bundle | Patient Satisfaction | Clinical Pathways | Product Life-Cycle Costs |
| Procedure & Episode Initiatives | Standardization | Physician Satisfaction | Education | Identifying Preventable Harm |
| Waste Management | Supply Formulary | Care Pathways | Cost Avoidance | Price Leveling |
| Employee Health | Infection Prevention | Safety | Length of Stay | |
| Environmental Sustainability | Antibiotic Stewardship | Readmissions | SKU reduction |
“The best part of building the CSO Program has been the transformation from a small group that had to focus on daily operations, to our current group that is approaching value from all angles while moving towards full clinical integration. The team has taken a blank slate and started to develop a strategy that is truly unique for our Health System.”
– Mark Walterbach, RN, System Senior Director, Supply Chain Management & Administration
“Emphasizing a collaborative approach between Supply Chain and physician representation allows for the ability to be innovative as an academic institution as well as financially responsible.”
– Sean C Kumer, PhD, MD
“Our Clinical Supply Optimization (CSO) program has spent its first two quarters aligning the right people, the right processes and the right systems to achieve our goals. This will require a cultural shift for our organization that we will continue to measure and continuously improve over time.”
– Angie Bruns, MHS, System Director, CSO